Burn your TV in your yard
And gather 'round it with your friends
And warm your hands upon the fire
And start again
Take the story you've been sold
The lies that justify the pain
The guilt that weighs upon your soul
And
throw 'em all away
People keep
asking why I am still here. Ebola is gone. Come home. The TV news said there
haven’t been any Ebola cases for weeks. The disease is defeated. The enemy
vanquished. Happy Christmas, War is Over was I think how John Lennon put it.
Victory. None of this is true. Burn your TV.
There was a
positive case just yesterday here in Monrovia. He died. During the last few
days of his life he was not recognized as an Ebola patient and came in contact
with hundreds of people in the community to include many healthcare workers.
The good news is no one has since popped up as positive from this event – yet –
and the system the government and partners have put in place to find people
that may have been exposed is working well. The process is called contact
tracing and it is perhaps the single most essential part of defeating this
disease. What it means is you have to find every single person that may have
been exposed to the infected person and at a minimum follow them on a daily
basis for the proverbial 21 days. In some cases, depending on the potential
severity of the exposure you may physically quarantine them. The teams here are
now quite skilled at contact tracing. And it works. When you so closely monitor
potential patients and isolate them the minute they start to appear ill it
markedly decreases the chance they will continue to pass along the infection.
All the virus wants to do is propagate, build a chain link by link. Contact
tracing stops the next link from even being built. Think of how many people you
come into contact with every day in your routine. Hundreds? Thousands?
Let’s explore the
word quarantine for a minute. We all know what it means. We hear it used on the
TV news, read about it in the papers but where does it come from? The word
"quarantine" originates from the Venetian dialect form of the Italian
quaranta giorni, meaning 'forty days'. This is due to the 40-day
isolation of ships and people before entering the city of Dubrovnik in Croatia.
This was a measure of disease prevention related to Black Death. Between 1348
and 1359, the Black Death wiped out an estimated 30% of Europe's population,
and a significant percentage of Asia's population. Just to refresh your memory,
the Black Plague was caused by bacteria that used fleas and rats as part of its
transmission cycle. Not nearly as exotic as Ebola which is a filovirus and
probably carried by bats but just as deadly back then. I have to remind you of
another part of the Black Plague’s history that you may not know. We are all
familiar with the children’s rhyme ring around the rosie, pocket full of posies,
ashes ashes we all fall down but we may not be aware that is all about the
Plague. The ring referred to a classic skin sign of infection, the pocket full
of posies was carried to mitigate the stench of death and the ashes and falling
down referred to the deaths. I am not sure if Ebola will birth its own nursery
rhymes. We’ll see.
The
original quarantine document from 1377 is kept in the Archives of Dubrovnik and
states that before entering the city newcomers had to spend 30 days -a trentine
- in a restricted place waiting to see whether the symptoms of Black Death would
develop. Later, isolation was prolonged to 40 days and called quarantine. Venice took the lead in measures
to check the spread of plague and appointed three guardians of public health in
the first years of the Black Death (1348). They enforced quarantine on ships at
harbor and even built quarantine facilities on small islands. Venice – such a
great city.
So
what happens when somebody gets Ebola? I’ll save the clinical talk for a different
time but let me walk you through how a patient is cared for. There are of
course many schools of thought - doctors are even worse than lawyers when it
comes to arguing - but there are established protocols that most agree on. A
patient showing symptoms gets to care sites in many different ways. If a person
is laying on the floor of their house or hut showing symptoms people know now
to contact the authorities. A specially trained and outfitted team and
ambulance goes and gets the patient. They know to bring them to an Ebola
Treatment Unit – an ETU. Patients may also show up on foot, via motorcycle or
even via wheelbarrow.
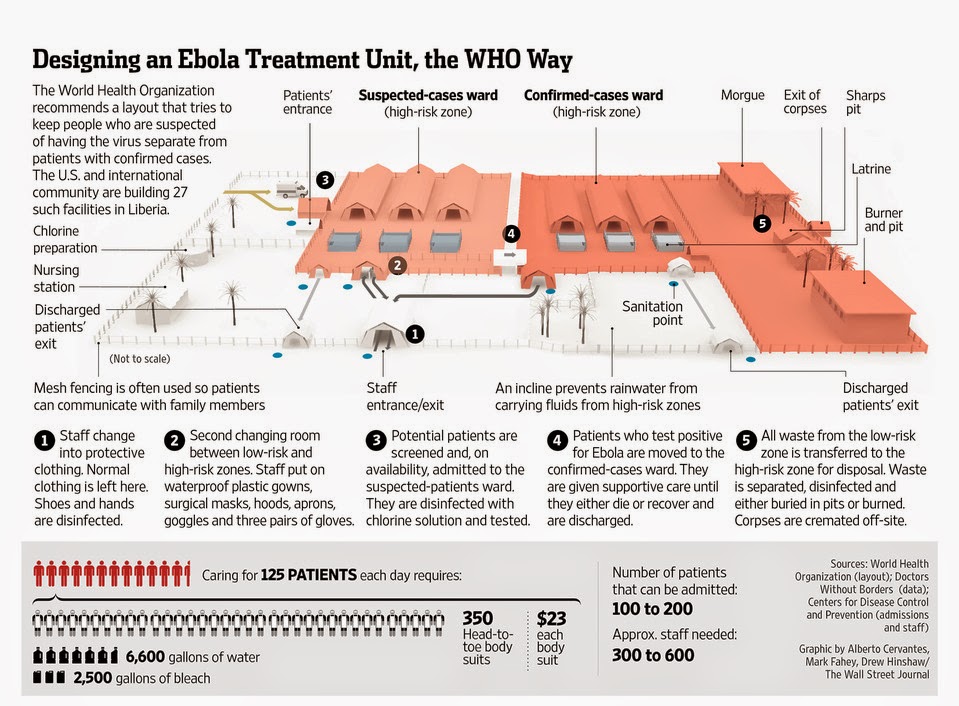
Once
at the ETU the patient begins to follow a very prescribed path that seeks to
isolate and protect the patient and protect the staff. The first part is
triage. There, across at least a meter or two of barrier separation, a quick
history is taken. The patients are guided on taking their own temperature with
an accurate digital thermometer. A judgment call is made right there whether or
not the patient fits the criteria. If so, a team in PPE (the spacesuits) comes
and escorts the patient into an area where they are cleaned and their
belongings gathered. They are now brought to a ward called the suspect ward.
Here they have a blood test drawn and samples are sent. The patient receives
what is called presumptive care at this point. Presumptive just means you
assume that everyone may also have malaria and infectious diarrhea – both very
common – and while you are waiting for the test to come back you may as well
treat these. Supportive care like nutrition and fluids are also given and of
course symptomatic care is given for fevers, pain and nausea for example.
It
may take a day or two for a test to come back. If it is positive the person is
moved to a completely new ward called the confirmed ward. Additional testing
takes place. More aggressive treatment continues. The same categories of care –
presumptive, supportive and symptomatic remain. Remember – there is no cure or
vaccine for Ebola – yet. There are very strict guidelines on how patients and
staff move and travel through the facility. One rule is there is no
backtracking. A patient will never go back to the suspect area once confirmed.
Remember some there in the suspect area may not have the disease. Likewise, a
staff member always travels from suspect to less infectious to most infectious
and does not backtrack either in order to minimize the chance of infecting
other patients. The whole patient and staff flow is exquisitely choreographed.
Those who went before us taught us.
Once
in the confirmed ward there are two possible patient outcomes. The patient
either survives and recovers or succumbs to the disease. If they recover there
is a protocol for confirming a disease free state and the patient is released.
They exit through a special area called Freedom’s Gate by some. They are given
the appropriate support to include the basics like bedding, clothing and food
since most everything was destroyed on arrival. No one is just sent out the
door. The communities have a well-established network of support facilities and
services. Still, a stigma surrounds Ebola survivors and many find it rough
going. It is not unlike that experienced by HIV patients back in the day.
Goodness, I just thought about my early days taking care of HIV/AIDS patients
back at San Francisco General in the early 80’s. It wasn’t even called AIDS. We
called it Gay Lymph Node Disease or Gay Related Immune Deficiency (GRID). We
were all so naïve but terrified. Again, the similarities are striking.
Many
patients die. Fatality rates range from 20-95% for Ebola. With good care in an
ETU setting the more favorable numbers play out. When a patient does die they
are treated with the utmost respect but again with very established protocols
for the handling of remains. A recently deceased body is highly highly
infectious. The ETUs all have proper morgues and a way to handle the remains. A
very special NGO called Global Communities has taken the lead throughout this
crisis for handling and burying remains. The ETUs transfer the deceased – again
protocols – to the Global Communities personnel who transport the patient for
burial. Every effort is made to include families in the process with appropriate
attention to infection control.
I
neglected to mention what happens to those in the suspect ward who prove
negative. Those who recover are similarly discharged with the appropriate
support. Those who remain ill are usually transferred to a more traditional
health care facility or clinic. For caregivers as mentioned there is a
similarly stringent workflow that starts with putting on the PPE – donning –
through to how to safely perform even the most routine tasks like an IV and
then when your shift is complete how to safely remove your PPE – doffing. I’ll
save the mechanics of all that for a different time as well.
A
couple of good video links give you an even better picture of what goes on
inside an ETU. The first link is of the MSF unit at ELWA3 in Monrovia. The
second is from another Liberian ETU.
I’ve
included some stock pictures of ETUs. You’ll note an abundance of concertina
wire and snow fence. No locals call it snow fence but those of us lucky enough
to have seen snow or even ski (how I miss it this season) do. The snow fence
and concertina wire are to help indeed demand one follows the traffic patterns.
No getting in (or out) unless appropriate. No backtracking. No left when you
should go right. Some ETUs are refurbished buildings or clinics that already
existed in the middle of a town. Some are just tents, although really good
tents, and plywood buildings in the middle of the jungle. They all operate in a
very similar fashion. They have all been critical to the success to date. Even
those that have not seen a patient act as fire stations ready to jump on any
ember. There’s still both smoke and fire. The house isn’t burning down anymore
but there is still work to do. Lots of it. Don’t believe everything you see or
read on the news. In fact, burn your TV in the yard. I haven’t seen TV in
months. I don’t really miss it. Ah, that’s a lie. I miss the John Oliver show
like crazy. How am I ever going to catch up?
Note: The lyrics to Throw it all Away are
by Toad the Wet Sprocket




 |
| Snow Fence |
 |
| Island Clinic ETU |

So interesting to hear about all of this - nothing on Ebola is on the news anymore. Jess and the girls are so proud of all that you are doing. Just amazing and seems like all the steps you put into place a working with the number of new cases on the decline. Can't wait to have you back in Hawaii!!!!
ReplyDeleteGood post - could get a great mental image, even before looking at the photos. Goodonya for including lyrics from Toad The Wet Sprocket. Good band!
ReplyDeleteGodspeed.
Linda